

Background: Allogeneic hematopoietic cell transplantation (allo-HCT) is the only curative therapy for patients with high-risk and refractory acute myeloid leukemia (AML). Unfortunately, up to 50 percent of patients relapse after allo-HCT.Recent research has shown that 30-50 percent of AML samples from patients relapsing after allo-HCT have downregulation of MHC class II (MHC-II) expression, which may promote immune effector evasion and disease relapse. These studies also report that interferon gamma (IFNγ) can restore MHC-II expression. IFNγ has never been systemically administered after allo-HCT and would likely cause significant and potentially life-threatening toxicities. Reinduction of MHC-II expression may lead to re-engagement of immune effectors, restoration of the graft-versus-malignancy effect, and disease control. We hypothesized that T cell immunotherapies targeting AML cells will lead to T cell activation, localized IFNγ release, and upregulation of MHC-II on AML cells.
Methods: For in vitro experiments, THP1 cells (THP1s), which have intermediate MHC-II expression, or primary human AML samples with low MHC-II expression from a patient relapsing after allo-HCT (AML-low cells) were co-cultured with or without T-cell immunotherapy and with or without human MHC-mismatched CD3+ T cells. The following T-cell immunotherapies were tested: flotetuzumab (FLZ), an investigational CD123 x CD3 bispecific DART® molecule; a CD33 x CD3 bispecific molecule (Creative Biolabs, Shirley, NY); and CD123-directed chimeric antigen receptor (CAR) T cells. THP1 IFNγ receptor-1 (IFNγR1) knockout cell lines were generated using CRISPR-Cas9. MHC-II expression was measured by flow cytometry and IFNγ concentrations via Luminex immunoflourescence assay. In order to rescue THP1s from FLZ-induced death and allow for longitudinal evaluation, a transwell plate system was used, placing THP1s, human CD3+ T cells, and FLZ in the top well and THP1s in the bottom well. This allowed for diffusion of IFNγ but not human T cells to the bottom wells, permitting MHC-II upregulation while limiting death. The upper and lower wells were coincubated together for 24 hours prior to harvesting of the THP1s in the lower well for longitudinal studies and mixed-lymphocyte reactions. For in vivo experiments, NOD-scid IL2Rgammanull mice expressing human IL-3, GM-CSF, and SCF (NSG-S) were irradiated with 250 rads and injected with 10e6 primary AML-low cells per mouse. After 5.5 weeks, mice were divided into the following groups: 1) untreated control; 2) FLZ only (2mg/kg); 3) human mismatched T cells only (10e7 T cells per mouse); 4) FLZ and T cells.
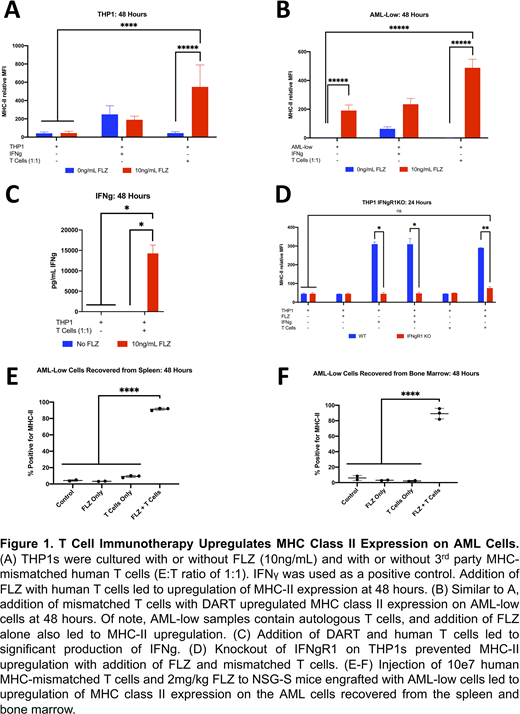
Results:In vitro co-culture of THP1 or AML-low cells with FLZ and T cells led to significantly increased MHC-II expression at 48 hours when compared with the control, FLZ only, and T cell only groups (Figure 1A-B). Co-culture of THP1s with the CD123 CAR-T cells led to similar results. Although co-incubation with a CD33 x CD3 bispecific led to a similar result, the MHC-II upregulation was not nearly as dramatic as that seen with CD123 targeting agents. Using a transwell system to rescue THP1s from FLZ-mediated toxicity, FLZ-induced MHC-II upregulation on THP1s peaked at 48-72 hours (similar kinetics to what is seen with IFNγ alone). These THP1s with upregulated MHC-II activated third-party donor mismatched human CD4+ T cells to a greater extent than untreated THP1s controls. Co-cultures of THP1s with CD4+ T cells and FLZ induced the secretion of very high concentrations of IFNγ, and blockade of IFNγ signaling through knockout of IFNγR1 led to abrogation of the effect (Figure 1C-D). Finally, in an in vivo model, NSG-S mice injected with AML-low samples and treated with FLZ and T cells showed significant upregulation of MHC-II expression on the AML cells. Single cell RNA-sequencing of AML cells purified from these mice is ongoing.
Conclusions: Use of FLZ and other T-cell immunotherapies targeting AML antigens led to both direct AML killing as well as significant upregulation of MHC-II expression on AML cells both in vitro and in vivo. The effect appears to be mediated primarily by IFNγ. T-cell immunotherapies represent a promising treatment approach for AML patients relapsing after allo-HCT and may lead to enhanced immune recognition in the 30-50% of patients who relapse after allo-HCT. Based on these results, a clinical trial treating patients relapsing after allo-HCT with FLZ is planned.
Christopher:Boulder Bioscience: Patents & Royalties: IP around the use of interferon gamma to treat stem cell transplant. Kim:Tmunity: Patents & Royalties: methods for gene editing in hematopoietic stem cells to enhance the therapeutic efficacy of antigen-specific immunotherapy (Licensed by University of Pennsylvania); Neoimmune Tech: Patents & Royalties: use of long-acting IL-7 analogs to enhance CAR T cells (licensed by Washington University). Muth:MacroGenics, Inc.: Current Employment, Current equity holder in publicly-traded company. Davidson:MacroGenics: Current Employment. DiPersio:Magenta Therapeutics: Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal